
Sarah Parks…gave still birth to a baby boy….a young doctor assisting the Parks’ regular physician begged for an opportunity to experiment with the idea he had to rouse the lifeless infant. A tub of ice was ordered and the young doctor plunged the baby into it. Out came the screaming little Parks and he was named Gordon after the doctor who prodded him to life’
Sir John Floyer, 1697
As the quote above shows, the use of cold water to stimulate the onset of respiration in depressed newborn infants started many years ago. However, it was James Miller from New Orleans and Bjorn Westin from Stockholm who in the 1950’s used cooling therapy for the purpose of resuscitating babies.
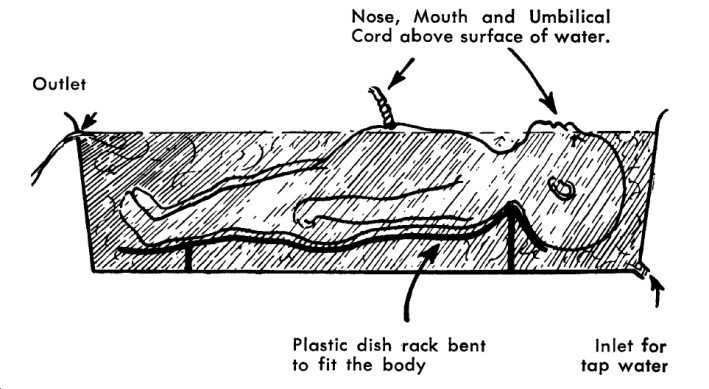
They described the use of hypothermia in infants with ‘asphyxia neonatorum’. Their study was on 10 severely depressed term infants who all had Apgar scores of 1 at birth and who had failed to respond to conventional methods of resuscitation. The apnoeic infants were immersed in a specially constructed cold water bath with the aim of reducing core temperature rapidly. Cooling was stopped when spontaneous respirations commenced or when the rectal temperature approached 27°C. One of the 10 infants died due to hyaline membrane disease but the remaining nine infants showed no neurological impairment or cerebral palsy at 10 years of age.
However, the importance of keeping all newborn infants warm overshadowed development in this field,
In the 1960s, clinicians saw hypothermia in newborn babies as something to be avoided.
The problem with infants who did not breathe at birth had been solved by the invention of mechanical ventilation, so any benefit of cooling was no longer needed. Secondly a significant study by Silverman showed that keeping small infants warm increased their survival and thus hypothermia was avoided.
Consequently, over the next two decades, studies of neonatal hypothermia in Europe and the USA were sporadic and often unsuccessful. After lying dormant for decades, it was not until the late 1980’s and early 1990’s that hypothermia as a neuroprotective strategy was revisited by Neonatal researchers.
A series of studies including CoolCap trial (2005,), NICHD trial (2005) and the TOBY trial (2009) demonstrated that both selective head cooling and whole body cooling was well tolerated in asphyxiated babies with minimal side effects.
The evidence from these randomised trials demonstrated that moderate hypothermia to 33°C–34°C for 72 hours initiated within 6 hours of delivery in infants with clear evidence of asphyxial encephalopathy reduces the risk of death or disability at 18–24 months of age and increases the rate of survival without disability.
Neonatal hypothermia has come a long way from the 1950’s when it was first introduced and the question arises as to where we would be now if the research had continued…